You are currently browsing the category archive for the ‘Resources’ category.
A person who knows of our interest in articles about depression lent us a magazine called MindFood. The May 2008 edition has a very youthful looking Madonna (the musician not the Mother of God) on the cover.
There were a couple of great articles in the latest version. A very good one by Findlay Macdonald telling how he succumbed to depression, which hopefully they will publish on their website later (we’ll link to it if they do).
Another was an interview with “genius” psychologist Dr. Dorothy Rowe who specialises in depression. She believes that depression is “not a physical illness to be treated with medication but a self-made prison you can leave, if you change the way you interpret your life.”
We had a look at the MindFood website and found this self-help article called Beat the Blues, by Donna Duggan. The article starts off:
There are myriad natural ways to beat the blues, lift your mood and improve your outlook, ranging from aroma-psychology to vitamins and minerals.
The section on breathing involves minimal equipment and makes the following suggestion:
No special technique is required – just take a few deep breaths when you need a break or can’t find the solution to a problem. Take a deep breath right into your stomach, hold it for a few moments, and then let the air go with a loud sigh. Deep breathing is one of the most effective mood boosters. In stressful situations many people hold their breath, or their breathing is very shallow, which restricts the flow of oxygen throughout the body and reduces mental function.
Workshop for Women
The Women’s Centre group called Depression or Expression has been highly recommended by our DSN group members. The group operates on the belief we suppress a lot of our feelings and that we need to learn safe and effective ways of expressing them. The group’s facilitator’s, Nilgun Kulpe and Mareile Stoppel, aim to create a supportive group environment, encourage creative expression, safe sharing with others and a start to the healing process.
The courses are held at Aranui High School and cost $20/$35.
For more details contact the Women’s Centre, Level 2, 134 Manchester Street. PO Box 13476, Christchurch 8141. Phone: (03) 379 7047
Step Ahead provides social, educational, recreational and prevocational rehabilitation through activity based programmes. Their aim is to enable people to live well in their community. Step Ahead contributes to a reality where anyone with a mental illness has access to the essentials for a life worth living. They run programmes in Stanmore Road, West, Rangiora, Amberley, Darfield and Ashburton.
Next Weeks Programme at Stanmore from their Whats on page is below:
Monday 10 March
10:00 Coffee Morning & 50c Morning Tea – Sausage Rolls (Helen)
10:30 Womens Group Picnic at Ashley Gorge – Bring lunch, togs, sunhat etc ($1.00)
1:00 Walking Group
Tuesday 11 March
10:00 Art with Selwyn ($2.00)
STAFF PLANNING AFTERNOON – STEP AHEAD CLOSED
5:00 Movies at Readings ($5.00)
Wednesday 12 March
9:15 Gym at Crichton Cobbers – Meet at Step Ahead ($2.00)
10:30 Rainbow Group
12:30 Lunch ($1.00)
1:00 Games Afternoon
1:00 Stack firewood at Step Ahead – Volunteers needed
1:15 Dietitian
Thursday 13 March
10:00 Walking Group
10:30 Meals on Wheels
10:30 All Day Stonecarving with Amberley ($4.00) – Bring your lunch
1:30 Swim/Relax at Centennial ($3.00)
1:30 Tennis
Friday 14 March
9:00 Tramp
9:30 Peer Support Training – Leave Step Ahead at 9.15am or meet at Holy Trinity Church Hall
10:15 Ten Pin Bowls ($4.50)
1:00 Sewing
- If you find yourself going through hell, keep going. Winston Churchill
- I start to think there really is no cure for depression, that happiness is an ongoing battle, and I wonder if it isn’t one I’ll have to fight for as long as I live. I wonder if it’s worth it. Elizabeth Wurtzel
- This is my depressed stance. When you’re depressed, it makes a lot of difference how you stand. The worst thing you can do is straighten up and hold your head high because then you’ll start to feel better. If you’re going to get any joy out of being depressed, you’ve got to stand like this. Charlie Brown
- Depression is the inability to construct a future. Rollo May
- Our greatest glory is not in never falling, but in rising everytime we fall. Confucius
- The term Clinical depression gets its way into many dialogues nowadays. One has the sense that a calamity has transpired in the supernatural background. Leonard Cohen
- Depression is merely anger without enthusiasm. Steven Wright
- I cry a lot. My emotions are very close to my surface. I don’t want to hold anything in so it it festers and turns into pus – a pustule of emotion that explodes into a festering cesspool of depression. Nicolas Cage
- You largely constructed your depression. It wasn’t given to you. Therefore, you can deconstruct it. Albert Ellis
- Depression is nourished by a lifetime of ungrieved and unforgiven hurts. Penelope Sweet
Imago Relationship Therapy was developed by Harville Hendrix and Helen LaKelly Hunt as a way for couples to extend themselves and grow as individuals and as a couple. They based it on their own experience of relationships, including their own marriage. Harville Hendrix often summarises the entire teachings of Imago in one simple phrase:
“You partner is another person – get it!”
Imago creates a safe framework that allows couple to really listen to each other. You get to know who their partner really is. Then it is possible to have deep, satisfying and above all real relationship.Imago techniques include a series of dialogue-based exercises. These exercises help you and your partner understand why you were first attracted to each other. Also why those initial reasons now draw you into a cycle of disagreement. The Imago Dialogue is a practical approach that helps achieve an authentic relationship with your partner.
The Imago Dialogue has three key components: mirroring, validation and empathy. Mirroring is when one person, the Sender, talks and the other, the Receiver, listens and then repeats the words just as they are said. This may seem easy until you try to do it. Often you will have reactions and responses that want to be aired. These defense mechanisms are automatic and come into play before you realise what is happening. It not enough to simply repeat someone’s words. The structured Imago dialogue uses simple questions such as “Did I get you?” and “Is There More?” to slow down the process and reduce reactivity. These simple phrases reinforce the sense of connection and invite the person talking to become more aware of their own thoughts and feel them.
Validation requires you to look through the eyes of the other. To see the world as it appears to them and to understand the other person’s point of view. Simply accepting that the other’s perception of the world is as valid as your own. In the empathy step, you imagine what your partner might be feeling. Feelings are simple words like “Angry, Sad, Lonely, Afraid, Happy, Joyful etc:”
Imago Relationship Therapy is made available through couples workshops, trained Imago therapists and in the books “Getting the Love You Want – A Guide for Couples” and “Keeping the Love You Find – A Guide for Singles” by Harville Hendrix. The Imago Dialogue is Copyright: Hunt/Hendrix and Imago Relationships International 2007.
Each of the three roles of the Winner’s Triangle; Vulnerable, Caring and Assertive, require the development of a different set of skills.
Vulnerable
Skill to be developed: Problem solving
Any technique that the Vulnerable person can use to get themselves thinking about options and consequences is valuable. The first set of the suggestions below are problem solving, self help initiatives. The second set are therapeutic techniques, suitable to group and individual work. The last group of suggestions are non-rescuing invitations that encourage problem solving.
Problem Solving
Training in problem solving techniques like:
- Working backwards
- Assess, Plan, Implement and Evaluate
- Trial and Error
- Lateral thinking
- Brainstorming
- Data collection
- Consulting feelings
Therapeutic
Therapeutic techniques to mobilise personal motivation and raise self-awareness.
- Guided fantasy
- Suggestion circle
- Two chair work
- Re-decision work
Non-rescuing invitations
Non-rescuing invitations to think about and solve problems
- What have you tried so far?
- How did that work?
- What do think went wrong?
- What do think went right?
- What will you do next?
- What do you predict as possible outcomes?
- How will you take care of yourself around negative consequences you envisage?
Caring
Skill to be developed: Listening
The development of listening skills that involve emphathising with the Vulnerable person is required. This might involve reflecting back to them as they speak what you are hearing them say and how they they are saying it, the underlying emotional tone. Interpretation and evaluation are avoided. Listening is frequently the only caring response needed.
The result of good listening is that the speaker experiences their feelings as having been honored and not discounted. Once you have established clear communication the following extras can be added in:
- Invitations to Problem Solving. (see above)
- Offers of specific practical help. The offers need to be genuine and not self-sacrificing
- Feedback about how you perceived them.
- Information. You may know some factual information that might assist the Vulnerable person.
Assertive
Skills to be developed: Assertiveness
Assertiveness is about getting your needs met without punishing. This requires:
- Asking for what you want
- Saying “no” to what you don’t want
- Giving feedback about behaviour that is causing a problem, and stating clearly what you want the other person to do differently
- Negotiating workable plans
- Using problem solving skills to get your needs met, even if the other person stays exactly the same
Based on a paper, ‘The Winner’s Triangle’, presented by Acey Choy of Sydney to the 1985 Transactional Analysis Conference held in Christchurch.
The Drama Triangle was originally developed in 1968 by Stephen Karpman, a Transactional Analysis trainer, as a way of graphically displaying the dance that occurs whenever we make someone else responsible for how we feel. According to Karpman, any time we don’t take responsibility for our feelings we are acting in a part of the Drama Triangle. The Drama Triangle can be a a simple yet powerful mechanism for understanding the relationships around a depressed person.
The roles of the drama triangle are: Victim, Persecutor and Rescuer. Karpman shows the relationship between these three roles by putting them on an upside down triangle. This shows the Persecutor and Rescuer in the one-up position that they take to the Victim.
- A Persecutor is someone who puts other people down and therefore goes one-up. They can act actively or be passive in response to the Victim.
- A Rescuer also goes one-up. They do more than their share and do they things they don’t really want to do.
- Victims don’t take responsibility for themselves. They will often feel overwhelmed with their feelings or even numb to them. They go one-down.
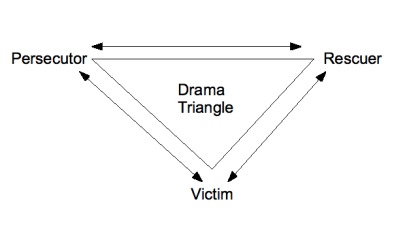
The arrows on the triangle indicate the direction of the transactions, but the drama in the Triangle comes from the switching of roles. As the drama triangle is played out, people change roles or tactics. Others in the triangle will then switch to match this. Sooner or later the Victim, sick of the one-down position, turns on the Rescuer. Or the Rescuer becomes fed up with a lack response or any appreciation of their efforts, becomes persecuting.
The Drama Triangle role names are part of our everyday language. Most people who are in relationship with depressed person will be familiar with being called a Rescuer when they are perceived as helping too much. A depressed person can also be labeled a Victim. While the Drama Triangle illustrates the problem quite clearly, its not always that easy to get out when you are in the middle of the drama. Thats why I like the Winner’s Triangle.
The Drama Triangle has been around long enough for there to be many derivatives and modifications. The Winner’s Triangle uses the same structure as the Drama Triangle but uses adult roles to replace the parent/child roles of the Drama Triangle. I first came across the Winner’s Triangle in a paper presented to the 1984 TA Conference by Acey Choy, she says she didn’t invent it and doesn’t know who did!

The roles of the Drama Triangle each have their equivalent role in the Winner’s Triangle. Each of the three roles in the Winner’s Triangle is an ‘OK’ role and requires the development of a different set of skills (see table below).
| Drama Triangle Role |
Winners Triangle Role |
Skill to be Developed |
| Victim | Vulnerable | Problem solving |
| Rescuer | Caring | Listening |
| Persecutor | Assertive | Assertiveness |
Any technique that the Vulnerable person can use to get themselves thinking about options and consequences is valuable. In the Caring role the development of listening skills that involve emphathising with the Vulnerable person is required. Listening is frequently the only Caring response needed. Assertiveness is about getting your needs met without punishing. Self awareness is essential in all three roles.
Links
Stephen Karpman’s own site
- Cut and arrange flowers or bring a live plant into your office or living space.
- Clean up your room (or start with one small shelf, drawer, or corner).
- Wash your clothes.
- Paint your walls a shade of yellow or another color that cheers you up.
- Try different kinds of music in your home – poppy, mellow, country, opera, pop, etc.
- Try aromatherapy – use different scents of candles, incense, or oils. Choose fragrances that remind you of a happy place or time or those that are known for their uplifting qualities.
- Move the furniture around to create a different feeling in a room.
- Change the lighting – try opening windows or curtains; if necessary, get full-spectrum light tubes
Five Questions to Answer before Seeing a Psychiatrist
- Have you had a thorough and satisfactory examination by a family practitioner and/or appropriate medical specialist before considering a psychiatrist?
- Have you obtained a second (or third, or fourth) opinion, and Are you prepared to be assertive, in questioning a psychiatrist’s diagnosis?
- Are you practicing poor health habits (drinking too much coffee, smoking cigarettes) or poor sleep habits that may be responsible for your not feeling like yourself?
- Are your feelings or behavior patterns normal reactions to life events (for example, pressure at work, loss of a loved one, etc.)?
- What medications, vitamins, or over-the-counter drugs are you currently taking?
Five Questions You Should Ask If You Do Go to a Psychiatrist
- Does your psychiatrist believe that DSM labels, such as “hyperactivity” and “depression”, are the same as real medical diagnoses, and does he or she base treatments on such labels.?
- Will your visit include an extensive medical history evaluation and physical examination, as well as appropriate laboratory tests?
- If your tests and examination reveal a biological disorder, will the drug your psychiatrist prescribes correct the problem or simply mask its symptoms?
- Is your psychiatrist recommending psychotherapy for your condition, and, ‘if so, Is the psychotherapy being prescribed in addition to medical diagnosis and treatment, or instead of medical diagnosis and treatment?
- How would your psychiatrist compare the risks and benefits of any drugs he or she recommends?
From “A Dose of Sanity” by Dr. Sydney Walker. Subtitled ‘A psychiatrist explains why why it’s not all in your head’, the book takes us inside the business of contemporary psychiatry and shows how, by sacrificing sound medical principles in favour of cook-book diagnosis and quick-fixes (like Ritalin and Prozac) depressed people’s health is being jeopardised.
If anti-psychotics aren’t working to help people recover from depression, maybe you should just ride with it. Is depression good for you?
“Don’t beat yourself up about being depressed, in most cases it will run its course” says Dr Paul Keedwell. Keedwell is an expert on mood disorders at the Institute of Psychiatry, King’s College London. He says that all people are vulnerable to depression in the face of stress to varying degrees, and always have been.
